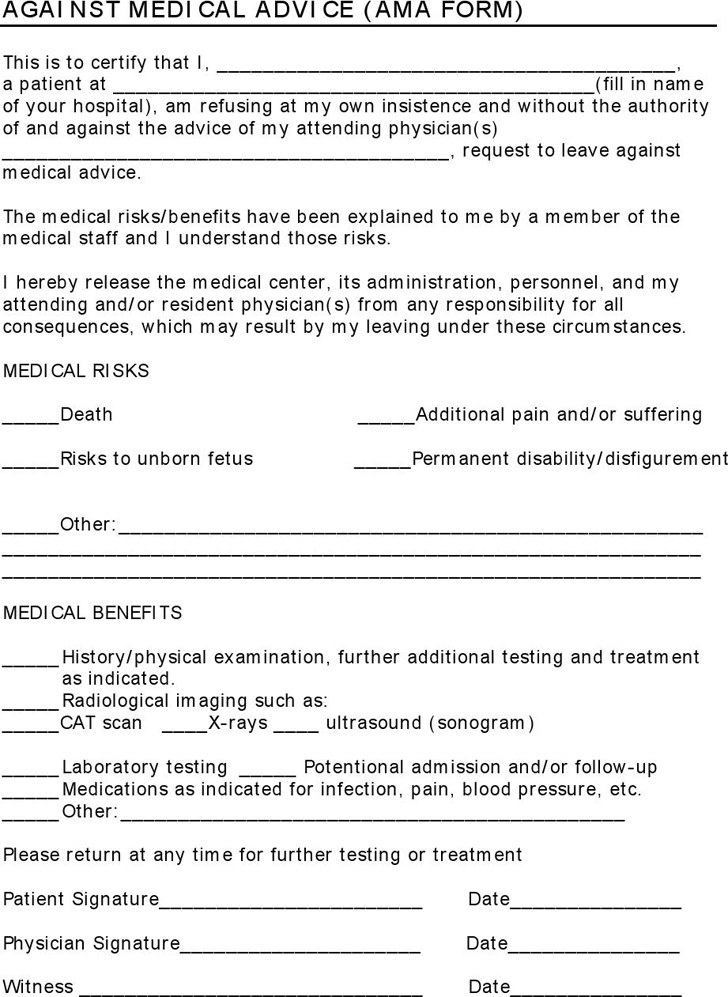
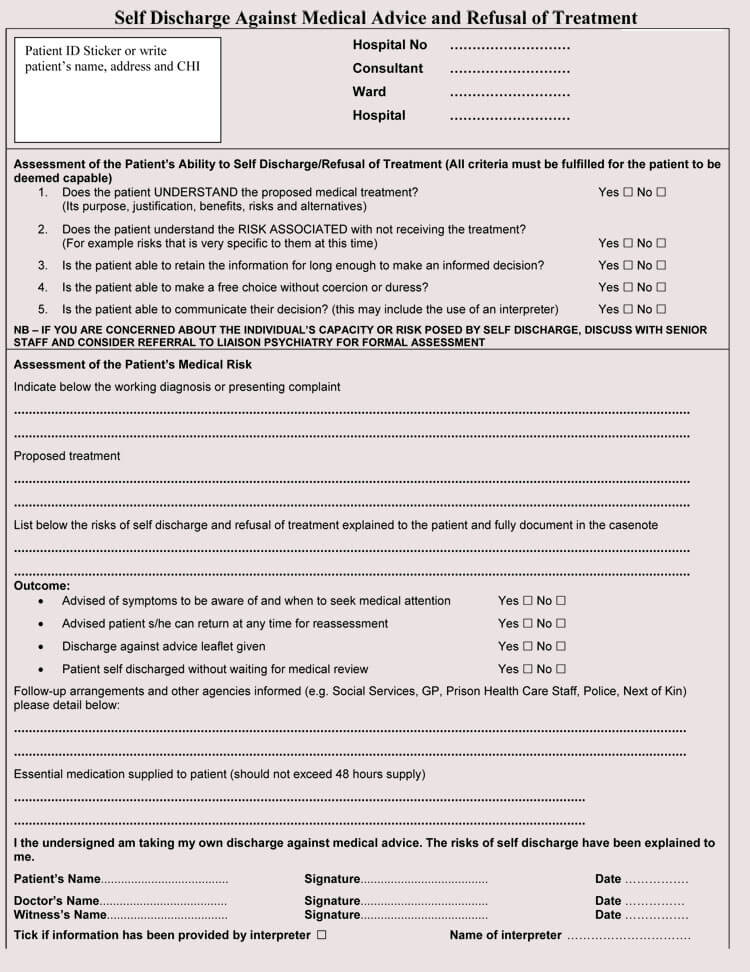
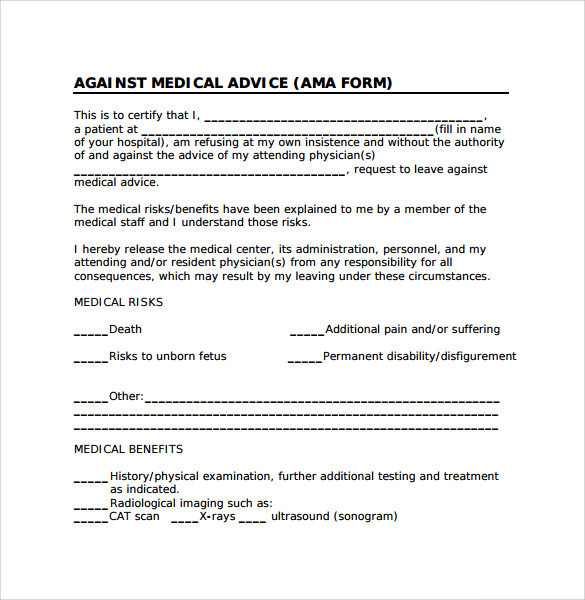
Printable Ama Form - I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the advice. Refusal of recommended treatment medical examination, treatment, or testing has been recommended for me. The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly.
The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the advice. Refusal of recommended treatment medical examination, treatment, or testing has been recommended for me.
The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the advice. Refusal of recommended treatment medical examination, treatment, or testing has been recommended for me.

Printable Ama Form Printable Forms Free Online
Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the advice. The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. Refusal of recommended treatment medical examination, treatment, or.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-26.jpg)
39 Printable Against Medical Advice [AMA] Forms
Refusal of recommended treatment medical examination, treatment, or testing has been recommended for me. The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. Form d this is to certify that i am over the.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-30.jpg)
39 Printable Against Medical Advice [AMA] Forms
Refusal of recommended treatment medical examination, treatment, or testing has been recommended for me. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-03.jpg)
39 Printable Against Medical Advice [AMA] Forms
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. Refusal of recommended treatment medical examination, treatment, or testing has been recommended for me. The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. Form d this is to certify that i am over the.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-16.jpg)
39 Printable Against Medical Advice [AMA] Forms
Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the advice. The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. I, __________________________________________, acknowledge that i have been informed.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-10.jpg)
39 Printable Against Medical Advice [AMA] Forms
Refusal of recommended treatment medical examination, treatment, or testing has been recommended for me. The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-02.jpg)
39 Printable Against Medical Advice [AMA] Forms
The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the advice. Refusal of recommended treatment medical examination, treatment, or.
Free Against Medical Advice (Ama Form) PDF 48KB 1 Page(s)
Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the advice. The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. Refusal of recommended treatment medical examination, treatment, or.
Printable Against Medical Advice Form Printable Forms Free Online
Refusal of recommended treatment medical examination, treatment, or testing has been recommended for me. Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and.
9 Against Medical Advice Forms Samples , Examples & Format Sample
The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. Refusal of recommended treatment medical examination, treatment, or testing has been recommended for me. Form d this is to certify that i am over the.
Refusal Of Recommended Treatment Medical Examination, Treatment, Or Testing Has Been Recommended For Me.
Form d this is to certify that i am over the age of 18 and i am refusing the services of this facility and i am leaving this facility against the advice. The purpose of an against medical advice (ama) form template is to protect both patients and healthcare providers by clearly. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the.